CEREBROVASCULAR CONDITIONS
Aneurysms
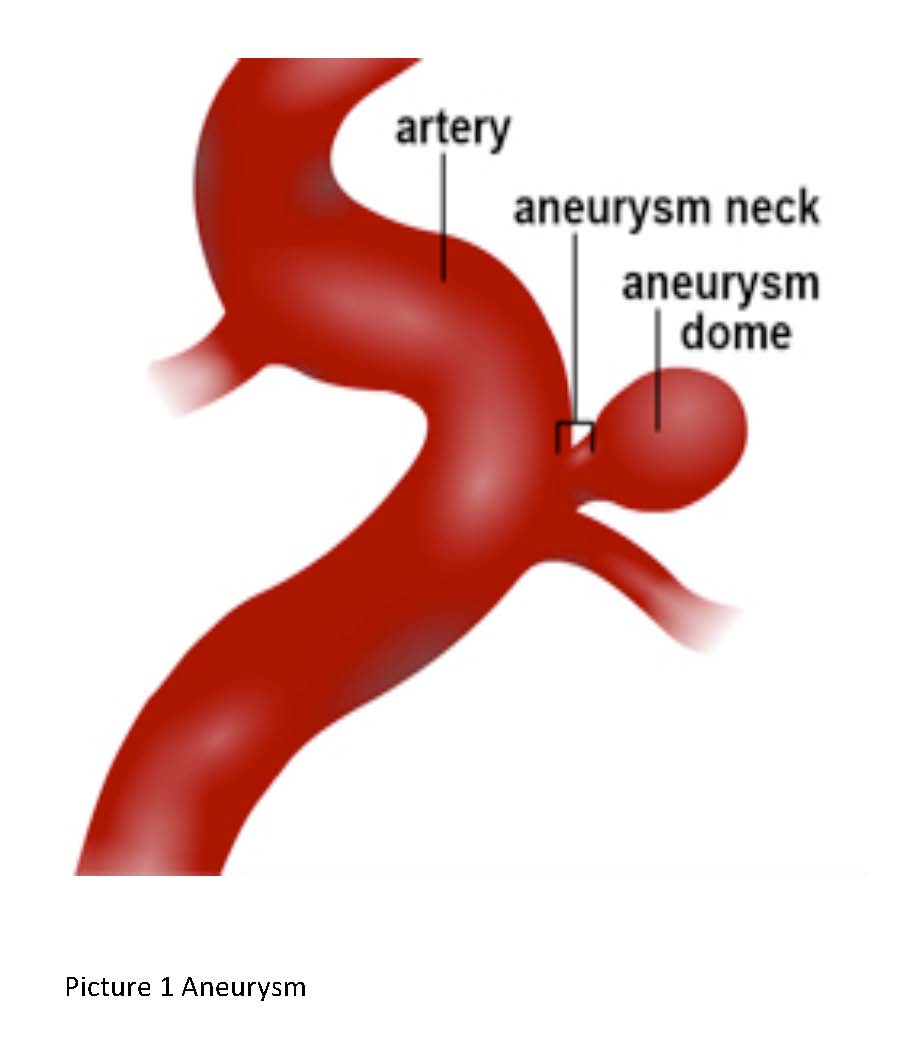
Click on picture to enlarge
A ruptured aneurysm is a serious condition. 1/3 of patients die and 1/3 develop severe neurological deficits. The risk of a second haemorrhage is high and is about 50% in the first 6 weeks. The diagnosis is made based on clinical symptoms and signs and confirmed by brain CT scan and occasionally lumbar puncture (Insertion of a small needle in the lower back to obtain cerebrospinal fluid). Patients will also require an angiogram (injection of contrast into the brain arteries via a catheter inserted into the main leg artery at the groin) to diagnose the aneurysm.
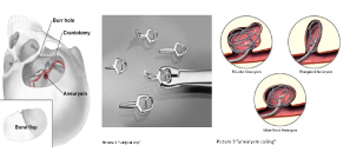
Click on picture to enlarge
The risk of haemorrhage from incidental unruptured aneurysms ranges 01-1% per year. The treatment options are observation with follow up angiograms, surgical clipping and endovascular embolisation. The choice of the best approach depends on the age of the patient, size and location of the aneurysm. Your surgeon will explain to you these options in more detail.
Arteriovenous malformation (AVM)
These are congenital vascular malformations characterised by thickened dilated arteries feeding a tangle of abnormal vessels (nidus) and draining into large veins. These are high flow shunts through which the blood drains from the arteries into veins bypassing the normal brain capillaries.
Patients present with intracranial haemorrhage (stroke), epilepsy, headaches and incidentally on brain CT scan.
AVM has 2-4% risk of haemorrhage every year and each haemorrhage carries 10% risk of death and 30% risk of major stroke. After the first haemorrhage the risk of a second haemorrhage in the first year increases to 6-18%.
AVM are classified into different grades based on their size, location and the nature of draining veins.
The diagnosis is confirmed by cerebral CT angiogram, MRI/MRA of the brain and formal cerebral angiogram
The treatment options include observation with follow up scans, surgical excision via craniotomy and focused radiation (stereotactic radiosurgery). Your surgeon will discuss with you these options in detail and explain the pros and cons of each approach.
Patients present with intracranial haemorrhage (stroke), epilepsy, headaches and incidentally on brain CT scan.
AVM has 2-4% risk of haemorrhage every year and each haemorrhage carries 10% risk of death and 30% risk of major stroke. After the first haemorrhage the risk of a second haemorrhage in the first year increases to 6-18%.
AVM are classified into different grades based on their size, location and the nature of draining veins.
The diagnosis is confirmed by cerebral CT angiogram, MRI/MRA of the brain and formal cerebral angiogram
The treatment options include observation with follow up scans, surgical excision via craniotomy and focused radiation (stereotactic radiosurgery). Your surgeon will discuss with you these options in detail and explain the pros and cons of each approach.
ALWAYS OBTAIN AN OPINION FROM YOUR TREATING DOCTOR ABOUT ANY MEDICAL CONDITION